

Background: Low-dose hypomethylating agents (HMAs) (azacitadine or decitabine) are safe and effective in patients with myelodysplastic syndromes (MDS). The aims of this study are to report the long-term follow-up of the phase 2 study of azacitidine or decitabine in lower-risk MDS and to identify specific populations of patients with lower-risk MDS who may benefit from early intervention with HMA therapy.
Methods: Patients with previously untreated MDS or chronic myelomonocytic leukemia with low or intermediate-1 risk by the international prognostic scoring system (IPSS) were randomized with a Bayesian response-adaptive design, and received either decitabine 20 mg/m2 daily or azacitidine 75 mg/m2 daily on days 1-3 every 28-day cycle. The primary efficacy end point is overall improvement rate (OIR: complete remission [CR], partial remission [PR], marrow CR [mCR], or hematologic improvement [HI]). Secondary end points are HI, transfusion independence, cytogenetic response, overall survival (OS), and time to acute myeloid leukemia or death. Overall survival (OS) was defined as the time duration from the start of therapy to the date of death from any cause or the date of last follow-up, whichever came first. A linear mixed effect model with fixed and random effect was assessed for the longitudinal repeated measurements of the percentage of blasts in bone marrow during the study treatment. Multivariate Cox regression analysis was performed to identify prognostic factors for survival after variable selection with a P-value cutoff of 0.250 by univariate analysis. Historical comparison was performed to identify subgroups of patients who had benefit from HMA therapy.
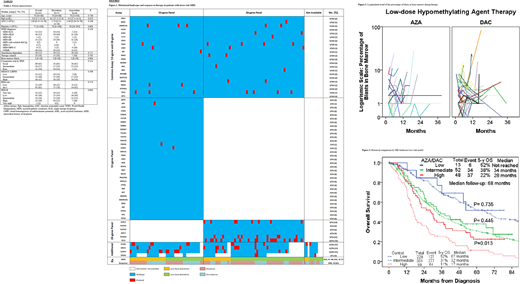
Results: Between November 12, 2012 and February 15, 2016, 113 patients were enrolled and treated with a median follow-up of 59 months: 73 (65%) patients were treated with decitabine and 40 (35%) were treated with azacitadine (Table 1; Figure 1). The median time from MDS diagnosis to the first date of therapy was 1.4 months (range, 0.2-49.8) and 0.9 months (range, 0.3-62.5) in the decitabine and azacitidine groups, respectively (P=0.052). The overall response rate was 67% and 48% in the decitabine and azacitidine groups, respectively (P=0.042); among 59 patients with baseline transfusion dependency, 19 (32%) achieved transfusion independence [decitabine, 16/39 (41%); azacitidine, 3/20 (15%); P=0.039]. The linear mixed effect model showed the equivalent longitudinal estimation of the percentage of blasts during the study (azacitadine vs. decitabine: P=0.989; estimate, -0.015; 95% CI, -2.325 - 2.295) (Figure 2). The median OS were 30 months and 37 months in the azacitadine and decitabine, respectively (P=0.625); the 5-year OS rates were 32% and 33%, respectively. By MD Anderson low-risk prognostic scoring system (MDA-LR-PSS), the median OS were not reached, 34 months, and 28 months in the low-, intermediate-, and high-risk groups, respectively (P<0.001); the 5-year OS rates were 52%, 38%, and 22%, respectively (Figure 3).
Multivariate analysis identified prior history of cytotoxic chemotherapy or radiation (P=0.002; hazard ratio [HR], 2.665; 95% confidence interval [CI], 1.436-4.944), transfusion dependency (P=0.016; HR, 2.023; 95% CI, 1.143-4.944), mutations in DNMT3A (P=0.006; HR, 4.266; 95% CI, 1.509-12.062), TP53 (P<0.001; HR, 5.594; 95% CI, 2.198-14.234), U2AF1 (P=0.018; HR, 2.263; 95% CI, 1.153-4.442), and complete response to HMA therapy (P<0.001; HR, 0.295; 95% CI, 0.154-0.568) as prognostic factors for survival. Type of HMA therapy was not prognostic factor for survival by univariate analysis (P=0.625; HR, 0.891; 95% CI, 0.559-1.418). When compared with a historical control cohort of 648 patients with low/intermediate-1 risk IPSS not treated with frontline HMAs, the survival improvement with low-dose HMA was notable in the high-risk cohort by MDA-LR-PSS (P=0.014; HR, 0.597; 95% CI, 0.396-0.900).
Conclusion: Low-dose HMA therapy can achieve transfusion independency in transfusion-dependent patients with lower-risk MDS, and can improve survival compared to historical data in patients with high-risk features by the MDA-LR-PSS.
Sasaki:Otsuka: Honoraria; Novartis: Consultancy, Research Funding; Daiichi Sankyo: Consultancy; Pfizer Japan: Consultancy. Jabbour:Genentech: Other: Advisory role, Research Funding; Adaptive Biotechnologies: Other: Advisory role, Research Funding; BMS: Other: Advisory role, Research Funding; Takeda: Other: Advisory role, Research Funding; Pfizer: Other: Advisory role, Research Funding; AbbVie: Other: Advisory role, Research Funding; Amgen: Other: Advisory role, Research Funding. Short:AstraZeneca: Consultancy; Amgen: Honoraria; Astellas: Research Funding; Takeda Oncology: Consultancy, Honoraria, Research Funding. Kadia:Ascentage: Research Funding; Cyclacel: Research Funding; Pulmotec: Research Funding; BMS: Honoraria, Research Funding; Genentech: Honoraria, Research Funding; Incyte: Research Funding; Celgene: Research Funding; Pfizer: Honoraria, Research Funding; Novartis: Honoraria; Abbvie: Honoraria, Research Funding; Amgen: Research Funding; JAZZ: Honoraria, Research Funding; Astellas: Research Funding; Astra Zeneca: Research Funding; Cellenkos: Research Funding. Borthakur:Nkarta Therapeutics: Consultancy; Jannsen: Research Funding; Treadwell Therapeutics: Consultancy; BioLine Rx: Research Funding; GSK: Research Funding; Novartis: Research Funding; PTC Therapeutics: Research Funding; PTC Therapeutics: Consultancy; Abbvie: Research Funding; Argenx: Consultancy; FTC Therapeutics: Consultancy; BMS: Research Funding; AstraZeneca: Research Funding; Polaris: Research Funding; Xbiotech USA: Research Funding; Oncoceutics: Research Funding; Incyte: Research Funding; BioTherix: Consultancy; BioLine Rx: Consultancy; Cyclacel: Research Funding; Curio Science LLC: Consultancy. Pemmaraju:DAVA Oncology: Honoraria; Daiichi Sankyo: Research Funding; Samus Therapeutics: Research Funding; Pacylex Pharmaceuticals: Consultancy; Cellectis: Research Funding; MustangBio: Honoraria; Affymetrix: Other: Grant Support, Research Funding; Plexxikon: Research Funding; Stemline Therapeutics: Honoraria, Research Funding; Novartis: Honoraria, Research Funding; Celgene: Honoraria; Incyte Corporation: Honoraria; AbbVie: Honoraria, Research Funding; SagerStrong Foundation: Other: Grant Support; LFB Biotechnologies: Honoraria; Blueprint Medicines: Honoraria; Roche Diagnostics: Honoraria. Cortes:Immunogen: Research Funding; Merus: Research Funding; Jazz Pharmaceuticals: Consultancy, Research Funding; Bristol-Myers Squibb: Research Funding; BiolineRx: Consultancy, Research Funding; Arog: Research Funding; Amphivena Therapeutics: Research Funding; Astellas: Research Funding; Novartis: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; Takeda: Consultancy, Research Funding; Sun Pharma: Research Funding; BioPath Holdings: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Telios: Research Funding; Daiichi Sankyo: Consultancy, Research Funding. Ravandi:Astellas: Consultancy, Honoraria, Research Funding; Orsenix: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy, Honoraria, Research Funding; Macrogenics: Research Funding; AstraZeneca: Consultancy, Honoraria; Xencor: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding; BMS: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria; Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding. Alvarado:BerGenBio ASA: Research Funding; Jazz Pharmaceuticals: Research Funding; Sun Pharma: Research Funding; FibroGen: Research Funding; Daiichi-Sankyo: Research Funding; Astex Pharmaceuticals: Research Funding; MEI Pharma: Research Funding; Tolero Pharmaceuticals: Research Funding. Kantarjian:BioAscend: Honoraria; Delta Fly: Honoraria; Janssen: Honoraria; Pfizer: Honoraria, Research Funding; Amgen: Honoraria, Research Funding; Immunogen: Research Funding; Novartis: Honoraria, Research Funding; Jazz: Research Funding; Daiichi-Sankyo: Honoraria, Research Funding; Oxford Biomedical: Honoraria; Abbvie: Honoraria, Research Funding; BMS: Research Funding; Ascentage: Research Funding; Adaptive biotechnologies: Honoraria; Aptitute Health: Honoraria; Sanofi: Research Funding; Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees. Garcia-Manero:Bristol-Myers Squibb: Consultancy, Research Funding; Genentech: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Onconova: Research Funding; Astex Pharmaceuticals: Consultancy, Honoraria, Research Funding; Merck: Research Funding; Novartis: Research Funding; Jazz Pharmaceuticals: Consultancy; Amphivena Therapeutics: Research Funding; Helsinn Therapeutics: Consultancy, Honoraria, Research Funding; Acceleron Pharmaceuticals: Consultancy, Honoraria; AbbVie: Honoraria, Research Funding; H3 Biomedicine: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal